Most people think of trauma as a single, dramatic event. A car accident. A violent attack. A natural disaster. But the experience of trauma is far more layered than any one moment, and its effects on the brain and body can persist for years, quietly shaping how a person thinks, feels, and moves through the world. Understanding those effects is the first step toward making sense of why trauma survivors respond the way they do, and why recovery is not simply a matter of moving on.
This article covers how trauma registers in the nervous system, what happens to the brain under prolonged stress, how symptoms tend to show up in daily life, and what the research says about recovery. Whether you are trying to understand your own experiences or support someone else, this overview offers a grounded starting point.
What Qualifies as Trauma
Trauma is not defined by the event itself but by the impact it has on the person who experiences it. Two people can go through the same situation and walk away with very different outcomes. One may recover relatively quickly. The other may carry lasting psychological and physiological changes. What matters is whether the event overwhelmed a person’s capacity to cope at the time it occurred.
Clinicians generally recognize two broad categories. Acute trauma stems from a single incident. Complex trauma, sometimes called developmental trauma, results from repeated or prolonged exposure to distressing events, often beginning in childhood. Situations that commonly produce complex trauma include childhood neglect, domestic violence, chronic illness, and ongoing community violence.
The Substance Abuse and Mental Health Services Administration has noted that more than two-thirds of children report experiencing at least one traumatic event by the age of 16. That figure gives some sense of how widespread traumatic stress actually is, even before accounting for adult experiences.
How the Brain Responds to Threat
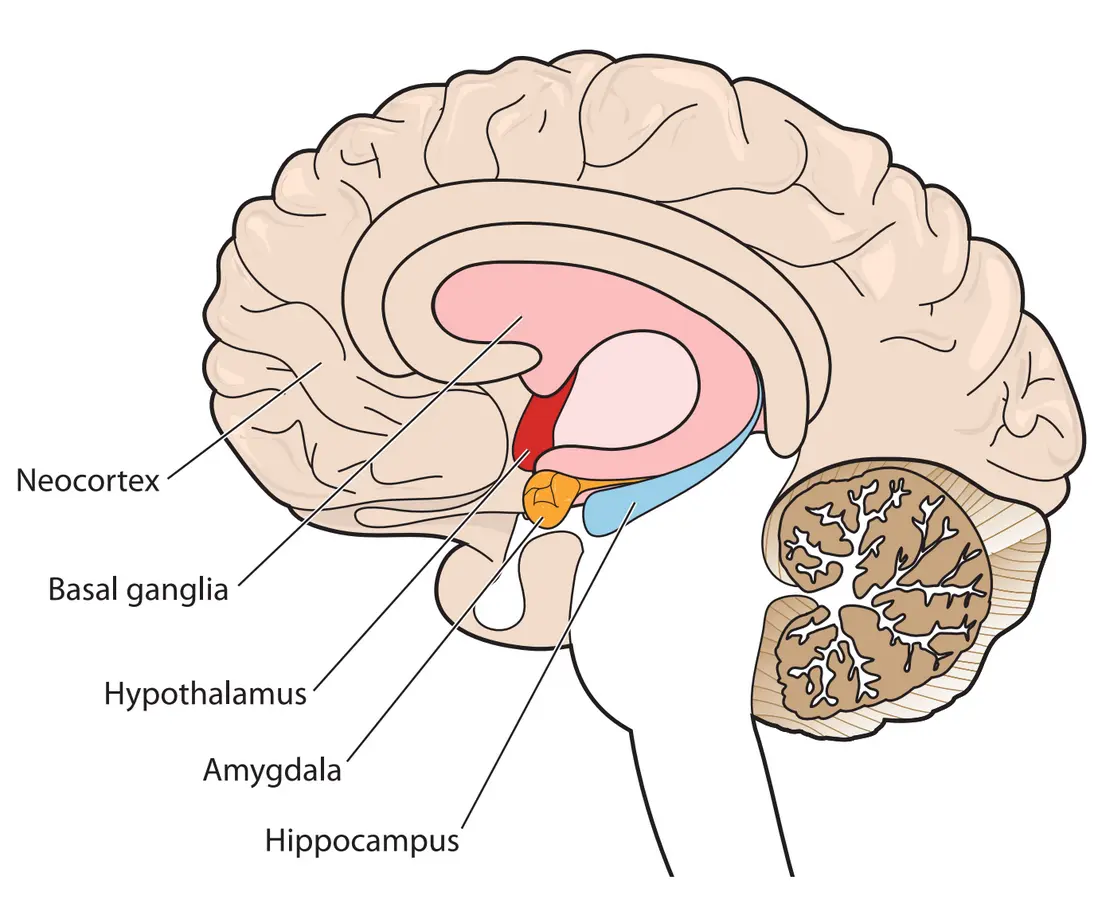
When a person perceives danger, the brain’s threat-detection system activates almost instantly. The amygdala, a small almond-shaped region deep in the brain, sends out an alarm signal. The hypothalamus then triggers the release of stress hormones, primarily cortisol and adrenaline, which prepare the body to fight, flee, or freeze. Heart rate increases. Muscles tense. Digestion slows. Attention narrows to the threat.
This cascade is adaptive in the short term. It is the reason humans have survived as a species. The problem arises when the threat response does not properly switch off after the danger has passed. In people who develop post-traumatic stress disorder, or PTSD, the brain can behave as though the threat is still present long after it has ended.
Neuroimaging research has shown that people with PTSD often display heightened activity in the amygdala and reduced activity in the prefrontal cortex, the region responsible for rational thinking, emotional regulation, and decision-making. This is one reason trauma survivors can struggle to feel safe even in objectively safe environments. The thinking brain is partially offline, and the survival brain is running the show.
The Role of the Hippocampus
The hippocampus plays a central role in memory formation and context. Under extreme stress, high levels of cortisol can impair hippocampal function, which helps explain why traumatic memories are often fragmented, nonlinear, or stored as sensory impressions rather than coherent narratives. A smell, a sound, or a particular quality of light can trigger a flood of sensory memory without a clear sense of where that memory belongs in time. This is not a sign of weakness or instability. It is a predictable result of how the brain processes overwhelming experiences.
Physical Symptoms That Often Go Unrecognized
Trauma is not only psychological. It lives in the body. Bessel van der Kolk, a psychiatrist and researcher who has spent decades studying trauma, made this argument central to his widely read work on the subject. Chronic muscle tension, sleep disturbances, gastrointestinal problems, fatigue, and a heightened startle response are all common physical manifestations of unresolved traumatic stress.
People with complex trauma histories are also more likely to experience chronic pain conditions and autoimmune disorders. Some researchers have linked this to the long-term effects of elevated cortisol on immune function and inflammation. A 2019 study published in JAMA Network Open found that adverse childhood experiences were significantly associated with a higher risk of chronic conditions including heart disease and diabetes in adulthood.
This connection between early trauma and physical health is sometimes referred to as the allostatic load, the cumulative wear on the body produced by prolonged or repeated stress responses. It is one reason that trauma is increasingly understood as a public health issue rather than a purely mental health concern.
Common Symptoms Across Trauma Types
Symptoms of traumatic stress can look very different from person to person, which is part of why they are often missed or misattributed. The following table outlines common symptom categories and how they tend to appear.
| Symptom Category | Common Presentations |
| Re-experiencing | Flashbacks, intrusive memories, nightmares, emotional reactions to reminders |
| Avoidance | Avoiding places, people, or thoughts connected to the event; emotional numbing |
| Hyperarousal | Difficulty sleeping, irritability, exaggerated startle response, difficulty concentrating |
| Negative cognition | Persistent shame, guilt, distorted self-blame, feeling permanently damaged |
| Dissociation | Feeling detached from one’s body, memory gaps, sense of unreality |
It is worth noting that not everyone who experiences trauma will develop PTSD. Some people develop other presentations, including depression, anxiety disorders, substance use disorders, or complex PTSD, which includes additional features such as difficulties with emotional regulation and interpersonal relationships. The presence of a supportive environment following trauma, access to resources, and prior history all influence how symptoms take shape.
What Recovery Actually Looks Like
Recovery from trauma is not a straight line, and it does not look the same for everyone. For some people, symptoms diminish naturally over weeks or months with the support of safe relationships and stable circumstances. For others, professional help is necessary to process experiences that the mind and body have been unable to integrate on their own.
Several evidence-based approaches have strong research support. Prolonged exposure therapy works by helping individuals gradually face memories and situations they have been avoiding, reducing the fear response over time. Cognitive processing therapy focuses on identifying and challenging distorted beliefs that formed as a result of the trauma. Eye movement desensitization and reprocessing, known as EMDR, uses guided bilateral stimulation to help the brain process stuck memories in a new way. Somatic approaches address the body’s stored responses directly through movement, breath, and physical awareness.
Clinicians who specialize in treating trauma typically draw from more than one of these frameworks, tailoring the approach to the individual’s history, symptoms, and readiness for different kinds of work. There is no single method that works for everyone, and good trauma care tends to be flexible and paced to the client.
Recovery also depends heavily on what researchers call the therapeutic relationship, the quality of trust and safety between a person and their clinician. Studies consistently show that this relationship is one of the strongest predictors of treatment outcomes across mental health conditions, and it matters even more in trauma work, where safety is often exactly what has been disrupted.
Factors That Support Healing
Beyond formal treatment, a number of factors contribute to resilience and recovery. Research on post-traumatic growth has shown that many survivors report meaningful positive changes following trauma, including deeper relationships, greater appreciation for life, and a stronger sense of personal strength. This does not minimize the suffering involved. It simply reflects the brain’s remarkable capacity for adaptation.
- Social connection: Having at least one trusted, consistent relationship is one of the most protective factors against long-term trauma effects.
- Physical safety: Recovery is difficult when a person remains in an unsafe environment. Stabilization comes before deeper processing.
- Routine and predictability: Consistent daily rhythms help regulate the nervous system and reduce baseline anxiety.
- Sleep: Restorative sleep is critical for emotional processing and memory consolidation. Sleep disruption both results from and worsens trauma symptoms.
- Meaning-making: Finding a way to integrate an experience into one’s larger life narrative, without forcing acceptance, is associated with better long-term outcomes.
- Access to care: Early intervention following traumatic events significantly reduces the likelihood of chronic PTSD developing.
Trauma affects a substantial portion of the population, and its effects reach across physical health, mental health, relationships, and daily functioning. The science makes clear that these effects are real, measurable, and not a sign of personal failure. They are the predictable consequence of an overwhelmed nervous system doing its best to protect the person carrying it. Understanding that is not a small thing. It changes how survivors see themselves and how others can show up for them. And it opens the door to the kind of support that actually helps.




Leave a Comment